FHIR Implementation Roadmap: Migrating from HL7 V2 to FHIR
For decades, Health Level Seven Version 2 (HL7 V2) has been the standard for exchanging clinical data. Established in 1989, its principles have been used to build massive clinical archives; one university hospital, for example, accumulated a collection of 300 million datasets from over 50 data sources in the last 30 years. However, its text-based, rigid structure struggles to keep up with the demands of modern healthcare, which relies on real-time data from mobile apps, cloud platforms, and complex analytics tools. Fast Healthcare Interoperability Resources (FHIR) first appeared in 2014 when HL7 released it as a web focused standard. It lets developers share health data in a way that’s more adaptable, faster, and easier to work with than the older formats. For a health organization that wants to refresh its technical foundation while also improving patient care, switching from HL7 V2 to FHIR makes sense. This guide provides a detailed roadmap for the entire journey, beginning with the initial planning stage and finishing with the follow up tasks after the transition.
What is driving the move from HL7 V2 to FHIR?
The shift from HL7 V2 to FHIR is driven by the fundamental differences in their architecture and capabilities. Understanding these distinctions clarifies why so many organizations are planning this migration.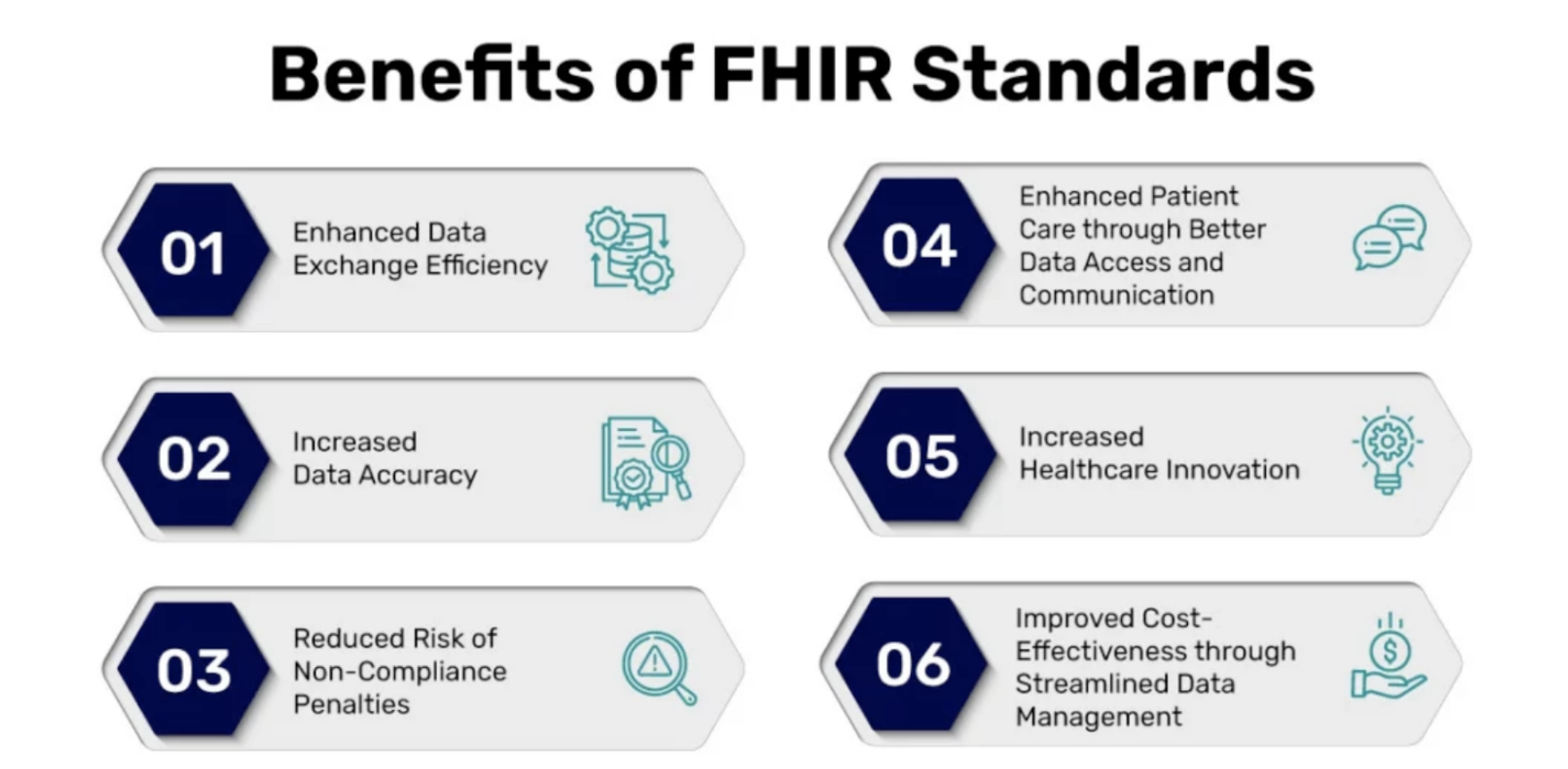 Source: Mind Bowser
Source: Mind Bowser
Why Healthcare Organizations Are Moving from HL7 V2 to FHIR
HL7 V2 was revolutionary for its time, but its limitations have become more apparent as technology has evolved. The standard’s flexibility often leads to inconsistent implementations and custom extensions ("Z-segments") that hinder true interoperability. Because it was designed before the widespread adoption of web APIs, V2 lacks support for the real-time, on-demand data access that modern applications require. FHIR was built to move past the roadblocks of earlier standards. It relies on familiar web technologies, like RESTful APIs, JSON, and XML, that make it easier for developers to implement and scale. Its growing adoption comes down to a few big advantages:- Better interoperability: FHIR’s resource-based design lets different systems, whether EHRs or patient apps, share data smoothly, helping eliminate the silos that older V2 setups created.
- Improved Data Flexibility: FHIR structures data into small, manageable pieces called "Resources" (for example, Patient, Observation, or Medication). These resources can handle a huge range of data types, including complex information like genomics and data collected from wearable fitness devices.
- Cost and Time Savings: Standardized APIs and a gentler learning curve reduce the need for costly, custom point-to-point interfaces, cutting development time and maintenance expenses.
Key Differences Between HL7 V2 and FHIR Standards
The technical distinctions and use cases between the two standards are significant. HL7 V2 works through messages built with pipe-and-hat delimited text, sending event-based updates whenever something changes. FHIR takes a different path: it’s resource-based and uses an API-driven model, so apps can request just the specific data they need instead of receiving a full document. HL7 V2’s strength has always been its flexibility, but that same trait often creates inconsistencies that make systems hard to connect. FHIR keeps the flexibility yet controls it through clear structure and defined extensions, so even customized elements can still work together smoothly. FHIR's modern foundation makes it inherently suited for the healthcare interoperability challenges of today, supporting everything from mobile apps to cloud-based analytics platforms.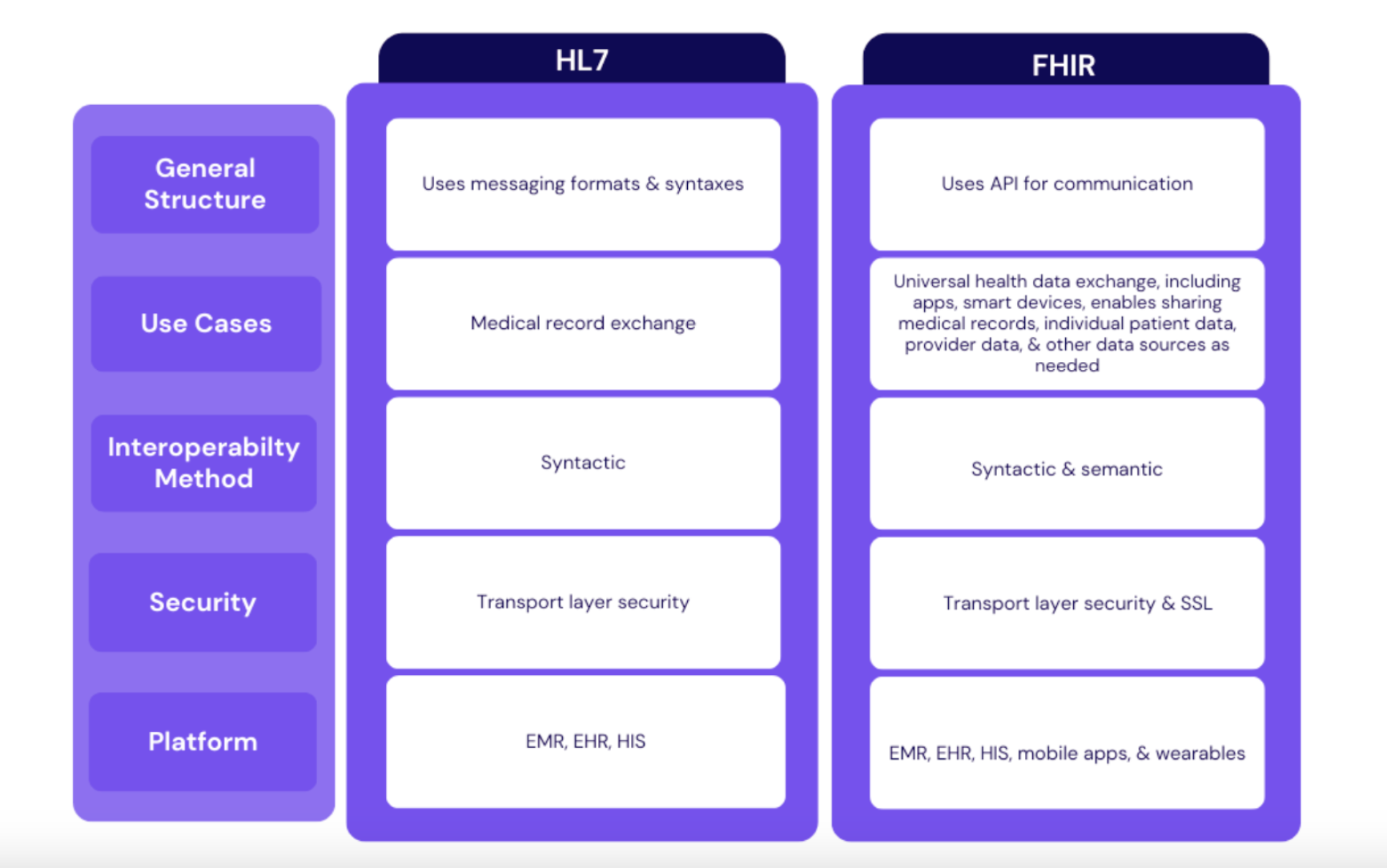 Source: TechVariable
Source: TechVariable
How do you plan for a successful migration?
Moving successfully from HL7 V2 to FHIR needs a careful plan that starts long before any programming or technical tasks begin. Taking the time for a detailed assessment and planning phase helps keep risks low and ensures the project matches what the organization is trying to achieve.Evaluating Your Current HL7 V2 Infrastructure
Begin by taking a close look at the environment you have right now. That means: Step 1. System Inventory: You must identify every system that currently relies on HL7 V2 messages. This means listing things like Electronic Health Records (EHRs), lab information systems (LIS), and platforms used for billing. Step 2. Data Flow Analysis: Sketch out which HL7 V2 messages are in play (for instance ADT for admissions or ORU for results) and follow the path those messages travel from one system to another. Step 3. Technical Readiness: Make sure your servers, networks, and integrations are capable of supporting APIs and the other web-based components FHIR depends on.Building Your FHIR Implementation Team
Assembling the right team is critical. A migration like this needs people with different skill sets working together. According to planning guides such as the Washington State Department of Health’s FHIR Roadmap, a solid team usually includes a Product Owner or Architect, a FHIR Specialist, Cloud DevOps and Services developers, a Project Manager, and Business and QA analysts. When internal expertise is limited, external partners with strong healthcare and technical backgrounds can help close gaps and guide the project strategically.Creating a Migration Timeline and Budget
Now that the assessment is finished, it’s time to sketch out the actual project. First, spell out what’s in scope and split the migration into bite size phases. A practical way to begin is with the basics, like patient demographics, then move on to the more intricate workflows once the foundation is solid. Next, put together a schedule you can actually meet and mark clear milestones along the way. Build a budget that covers software licenses, the developers who will write the code, and the training sessions your staff will need. Finally, think through what could go wrong, for example data loss, system downtime, or users pushing back, and decide in advance how you’ll deal with each issue.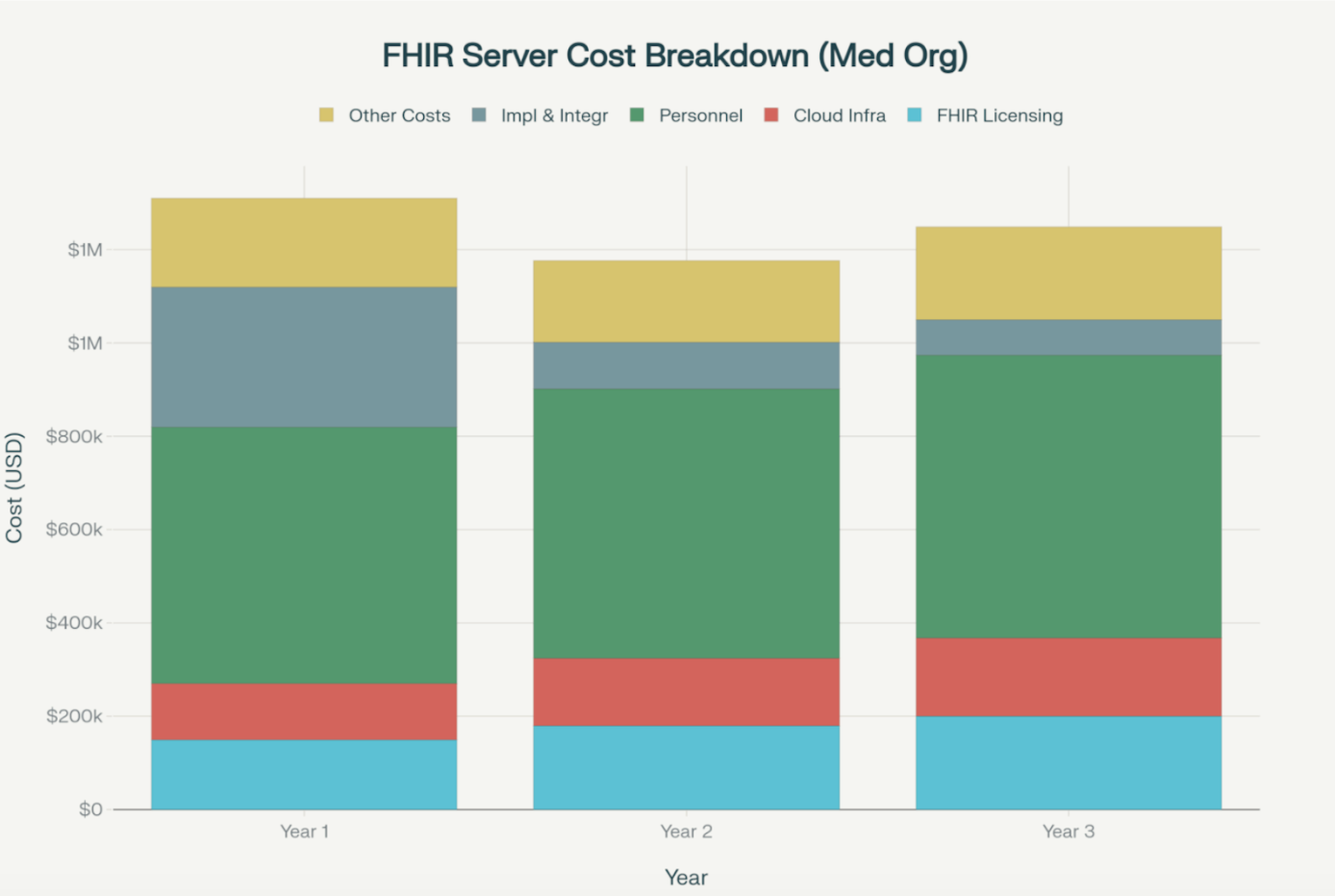 Source: WV United
Source: WV United
What does the FHIR implementation roadmap look like?
You can organize the migration into a set of sensible steps, starting with data charting and ending with the final launch. Every organization has a different path, but this step-by-step process offers a solid structure to follow.Phase 1: Data Mapping and Transformation Strategy
Getting this right is often the hardest and most important part of the migration. You have to translate data from the segment-based structure of HL7 V2 into the resource-based model used by FHIR. For instance, you would map a PID segment from a V2 message to a FHIR Patient resource. In the same way, OBX and OBR segments must be translated to Observation and Specimen resources. This is difficult because V2 messages are usually customized for each organization. They often have custom fields that aren't well documented. As an IOS Press study pointed out, moving a legacy archive means you finally have to deal with all the errors and exceptions the old system just ignored. Official HL7 guides and automated tools are helpful, but they aren't enough. You really need a data analyst who knows both standards well to handle the complexities and make sure the data stays accurate.Phase 2: Pilot Implementation and Testing
Avoid starting the full rollout right away. Run a pilot test with a limited scope first, such as in a single department or just for one workflow. This lets you test your mapping logic and integration tools in a safe environment. Use this time to test rigorously for data accuracy and system speed. You need to run checks to confirm that a V2 lab result matches its FHIR version perfectly. Also, simulate heavy traffic loads to make sure the system can handle busy periods without crashing.Phase 3: Executing the Full-Scale Migration
Once the pilot succeeds, you can move on to the full migration. It’s usually best to roll out in stages to minimize disruptions. Keep a close watch on speed and error rates throughout the rollout. This helps you spot and fix issues as soon as they pop up.Phase 4: Optimization and Maintenance After the Move
Going live doesn't mean the work is finished. You must keep monitoring the new FHIR infrastructure to make sure it keeps running smoothly. This involves fixing performance issues as they arise and planning ahead for future FHIR version upgrades so the system stays current.What are the key technical considerations for implementation?
A successful migration hinges on making the right technical choices regarding tools, security, and validation. Source: Mind Bowser
Source: Mind Bowser
FHIR Integration Services and Tools
There are many tools that can simplify the migration process. Integration engines can handle FHIR resources and transform data from older HL7 versions. Open-source libraries such as HAPI FHIR provide strong frameworks for managing and converting FHIR resources in Java. For cloud migrations, platforms like Google Cloud Healthcare API and Azure FHIR deliver secure, scalable environments for storing and processing FHIR data.Security and Compliance in FHIR Implementation
Security remains a top priority. FHIR comes with built-in safeguards such as role-based permissions and data encryption to keep patient information protected. Implementations should also use standards like OAuth 2.0 and SMART on FHIR to manage secure, authorized access, especially for third-party apps. Compliance with HIPAA and other regulations isn’t optional; it has to be part of the foundation of any FHIR implementation plan.Testing and Validation Methodologies
Thorough testing is essential to guarantee data integrity. Validation tools like the official FHIR Validator and Inferno help ensure that FHIR resources are correctly formatted and compliant with the relevant implementation guides.How can you overcome common migration challenges?
Migrating from a decades-old standard is rarely straightforward. Anticipating common hurdles can help you develop effective solutions.Data Quality and Consistency Issues
Data quality is one of the biggest hurdles in any migration. HL7 V2 messages can contain “unknown” fields or unclear values that take serious digging to understand. The most reliable way to avoid data loss or corruption is to combine thorough data cleaning and validation with automated mapping tools and hands-on expert checks.Legacy System Integration Challenges
Connecting modern FHIR infrastructure with legacy systems that may not be compatible is a significant obstacle. A report on the University Hospital of Giessen’s migration highlights this, describing the difficulty of moving data from a 30-year-old clinical archive. The solution often involves using middleware to act as a bridge or developing a phased migration that allows legacy and modern systems to coexist during the transition. For more on this topic, see this article on inside EHR integration.Staff Training and Change Management
Technical challenges are only part of the story. Clinicians and IT teams accustomed to HL7 V2 workflows may resist the change. A proactive change management plan is essential.How Kanda Can Help
The move from HL7 V2 to FHIR reshapes how healthcare systems share and manage information. It’s a challenging process that blends technical precision with strategic planning, requiring teams to secure data, connect outdated systems, and meet every compliance benchmark. Kanda Software can help you:- Build Custom Platforms: Develop secure, scalable, and compliant FHIR-based software and APIs tailored to your specific clinical and operational needs.
- Manage Legacy System Integration: Create effective data transformation pipelines and middleware to bridge the gap between older HL7 V2 systems and modern, cloud-based platforms.
- Develop Interoperable Applications: Design and build powerful analytics dashboards, clinical support tools, and patient-facing applications that unlock the full value of your health data.
- Ensure Security and Compliance: Engineer platforms to meet strict regulatory standards like HIPAA, protecting your data and your organization at every step of the migration process.
Conclusion
The healthcare industry is shifting from the constraints of older, message-based standards to the possibilities of connected, API-driven platforms. Legacy applications built on HL7 V2 remain indispensable for day‑to‑day operations, yet the path forward involves adopting software that is secure, can scale to meet demand, and integrates seamlessly across the whole digital‑health ecosystem. For healthcare organizations, the goal is not a complete overhaul in one move but a strategic migration that links established systems to the networked capabilities ahead. By adopting a modern FHIR implementation approach, the industry can harness its data more effectively and speed the delivery of safer, more powerful treatments around the world.Related Articles

CMS Prior Authorization Rule 2026: What Health Systems and Payers Actually Need to Build by October 2027
Key Takeaways The 2026 CMS Prior Authorization (CMS-0062-P) rule extends electronic prior authorization requirements to drugs for the first time, closing a major gap left by the 2024 rule. The hard compliance deadline is October 1, 2027 - by that date, systems must be live, not in development or testing. Compliance requires three major technical…Learn More
Unlocking Actionable Insights from Medical Data with Clinical NLP
Key Takeaways Clinical NLP extracts useful details from notes, reports, and other free-text records so teams can work with them. The clearest use cases include coding support, trial matching, safety monitoring, registry work, and population health. The output is only useful if it connects to the standards healthcare teams already use: SNOMED CT, RxNorm, LOINC,…Learn More
Why Omics and Clinical Data Integration Remain a Challenge and How to Fix It
Key Takeaways Omics and clinical data often remain separate, making them harder to use together than they should be. The main challenge is usually not the data itself, but the mismatched formats, siloed systems, and disconnected teams surrounding it Addressing that requires robust infrastructure, shared standards, and workflows that hold up without constant manual intervention.…Learn More
AI Copilots in Healthcare: Minimizing Diagnostic Risks With Smart Virtual Assistants
Key Takeaways AI copilots act as always-on virtual assistants managing documentation, triage, and decision support so clinicians can focus on patients. With 12 million diagnostic errors and up to 80,000 deaths annually, AI copilots are built to catch what overloaded clinicians miss, not replace them. Dragon Copilot saves clinicians around 5 minutes per encounter with…Learn More

