July 10, 2025
Healthcare
FHIR vs. HL7: The Pros, Cons, and Use Cases
Effectively exchanging healthcare data is fundamental to modern medicine. For decades, getting different health IT systems to communicate without problems has been a major challenge. Two standards are at the heart of this issue: Health Level Seven (HL7) Version 2 and the newer Fast Healthcare Interoperability Resources (FHIR). They both seek to enable interoperability, yet they originate from different technological eras and are built on distinct philosophies.
Their impact is huge. An estimated 95% of U.S. healthcare organizations still use the workhorse standard, HL7 V2. Meanwhile, FHIR's growth is rapid. As of 2025, nearly 90% of global health systems have implemented FHIR-enabled APIs, and 84% of healthcare leaders expect that growth to continue.
This is more than a technical debate for IT teams. The choice of standard affects patient care, data security, and the ability to innovate with mobile health apps and AI-driven analytics. This article will examine the key differences between HL7 V2 and FHIR, covering their technical foundations, pros, cons, and specific use cases to clarify the healthcare data landscape.
 Source: Kodjin
HL7 V2 operates as a messaging standard based on an event-driven, point-to-point model. When a specific event happens, like a patient being admitted or a lab order being placed, one system creates a text-based message and sends it to another.
An HL7 V2 message is structured with segments and fields, using pipe-delimited (|) ASCII text. Key segments include:
Source: Kodjin
HL7 V2 operates as a messaging standard based on an event-driven, point-to-point model. When a specific event happens, like a patient being admitted or a lab order being placed, one system creates a text-based message and sends it to another.
An HL7 V2 message is structured with segments and fields, using pipe-delimited (|) ASCII text. Key segments include:
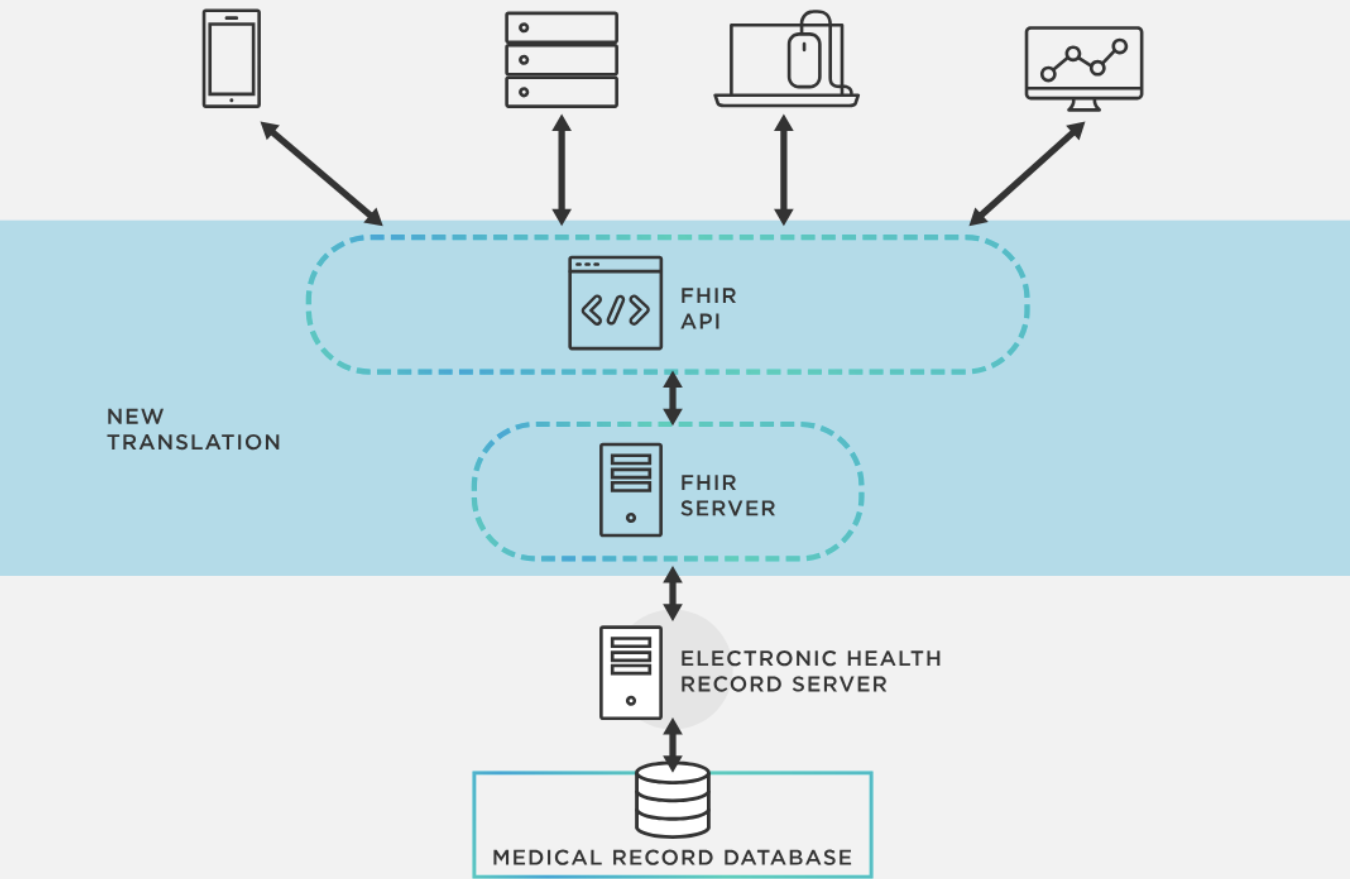 A diagram of the FHIR architecture, where a central API translates data from an electronic health record for secure use by modern applications like mobile apps and analytics tools.
Source: Tibco
FHIR breaks healthcare information into modular components called "resources." A resource is a self-contained unit of clinical or administrative data, like a patient, observation, medication, or encounter. These resources can be accessed, combined, and exchanged individually to support a wide range of uses.
FHIR's technology is its key differentiator. It uses the same open web technologies that run major e-commerce and social media platforms, including:
A diagram of the FHIR architecture, where a central API translates data from an electronic health record for secure use by modern applications like mobile apps and analytics tools.
Source: Tibco
FHIR breaks healthcare information into modular components called "resources." A resource is a self-contained unit of clinical or administrative data, like a patient, observation, medication, or encounter. These resources can be accessed, combined, and exchanged individually to support a wide range of uses.
FHIR's technology is its key differentiator. It uses the same open web technologies that run major e-commerce and social media platforms, including:
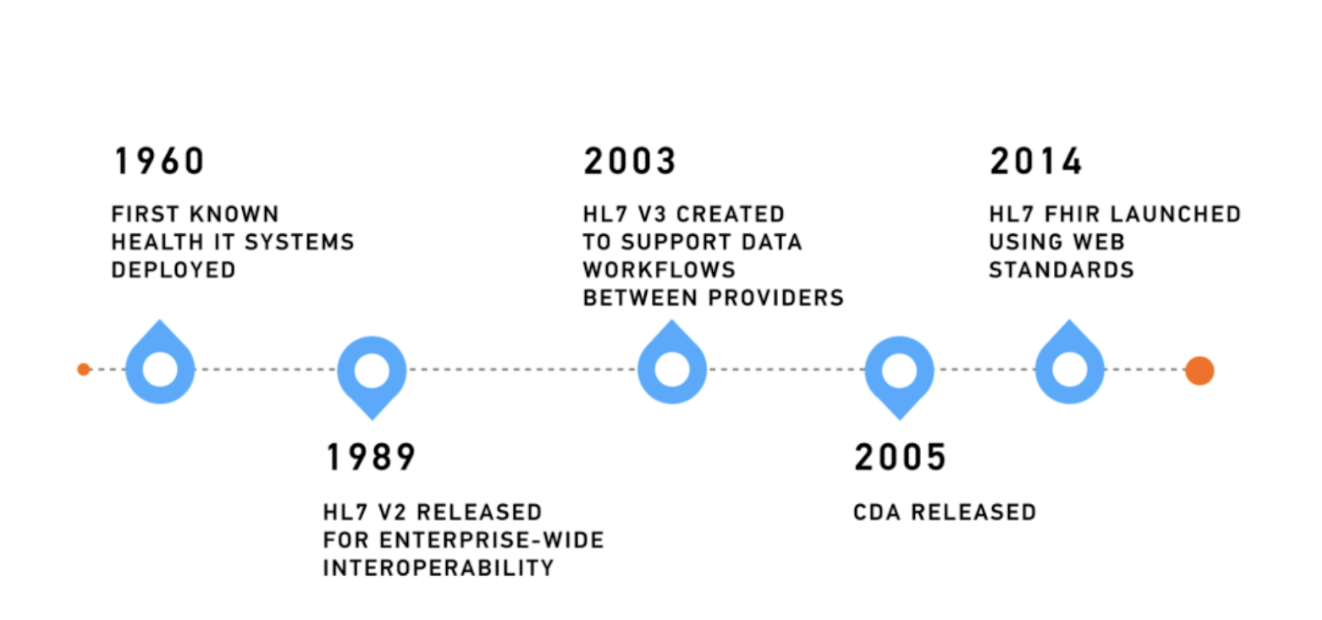
What is HL7 Version 2?
HL7 Version 2 (V2) appeared in the late 1980s to solve a major problem: getting different hospital information systems to communicate with one another. Before V2, connecting systems like a laboratory information system (LIS) to an electronic health record (EHR) meant building a custom, expensive interface for each link. HL7 V2 offered a common language that streamlined these connections and supported many clinical and administrative tasks.
Source: Kodjin
HL7 V2 operates as a messaging standard based on an event-driven, point-to-point model. When a specific event happens, like a patient being admitted or a lab order being placed, one system creates a text-based message and sends it to another.
An HL7 V2 message is structured with segments and fields, using pipe-delimited (|) ASCII text. Key segments include:
- MSH (Message Header): A required segment with information about the message itself, such as the sender, receiver, and message type.
- PID (Patient Identification): Contains the patient's demographic details, including name, date of birth, and medical record number.
- PV1 (Patient Visit): Includes details about a specific patient visit, such as the attending physician and location.
The Pros of HL7 V2
HL7 V2's main advantage is its long history and wide adoption. For over 30 years, it has been the primary standard for internal hospital communications. This longevity makes it highly reliable for high-volume, established workflows, particularly in labs and pharmacies. Most older EHRs and clinical systems have solid, built-in support for V2 messages, making it a fundamental part of existing infrastructure.The Cons and Limitations of HL7 V2
The flexibility that spurred V2's adoption is also its biggest flaw. The standard was designed for customization, which resulted in significant implementation inconsistencies. Two hospitals might use the same ADT-A01 message but format or interpret the data in different ways. This requires custom mapping for every new connection. Additionally, HL7 V2 has several technical weak points:- Point-to-Point Communication: It was designed for one-to-one connections and lacks support for the one-to-many data exchange needed by modern, interconnected systems.
- Limited Extensibility: Custom "Z-segments" can be added, but they are not standardized. This creates interoperability problems unless the sender provides manual explanations.
- Outdated Technology: HL7 V2 was created before the internet became common. It isn't designed for modern web services, mobile apps, or cloud platforms. It has a steep learning curve and requires specialized skills, which makes it challenging for new developers.
What is FHIR? The Modern Approach to Interoperability
HL7 International developed Fast Healthcare Interoperability Resources (FHIR) to address the shortcomings of older standards, launching it in 2014 FHIR (pronounced "fire") is a complete reimagining of health data exchange for the modern internet. It is still an HL7 standard, which is why it's called HL7 FHIR, but it's built on an entirely new technological foundation.
A diagram of the FHIR architecture, where a central API translates data from an electronic health record for secure use by modern applications like mobile apps and analytics tools.
Source: Tibco
FHIR breaks healthcare information into modular components called "resources." A resource is a self-contained unit of clinical or administrative data, like a patient, observation, medication, or encounter. These resources can be accessed, combined, and exchanged individually to support a wide range of uses.
FHIR's technology is its key differentiator. It uses the same open web technologies that run major e-commerce and social media platforms, including:
- RESTful APIs: Applications can request specific data from a server with standard HTTP commands (GET, POST, etc.). This replaces rigid point-to-point connections with a flexible, one-to-many model.
- JSON and XML: Data is represented in human-readable formats that most modern developers already know, greatly reducing the implementation barrier.
How Does FHIR Differ from HL7 V2? A Head-to-Head Comparison
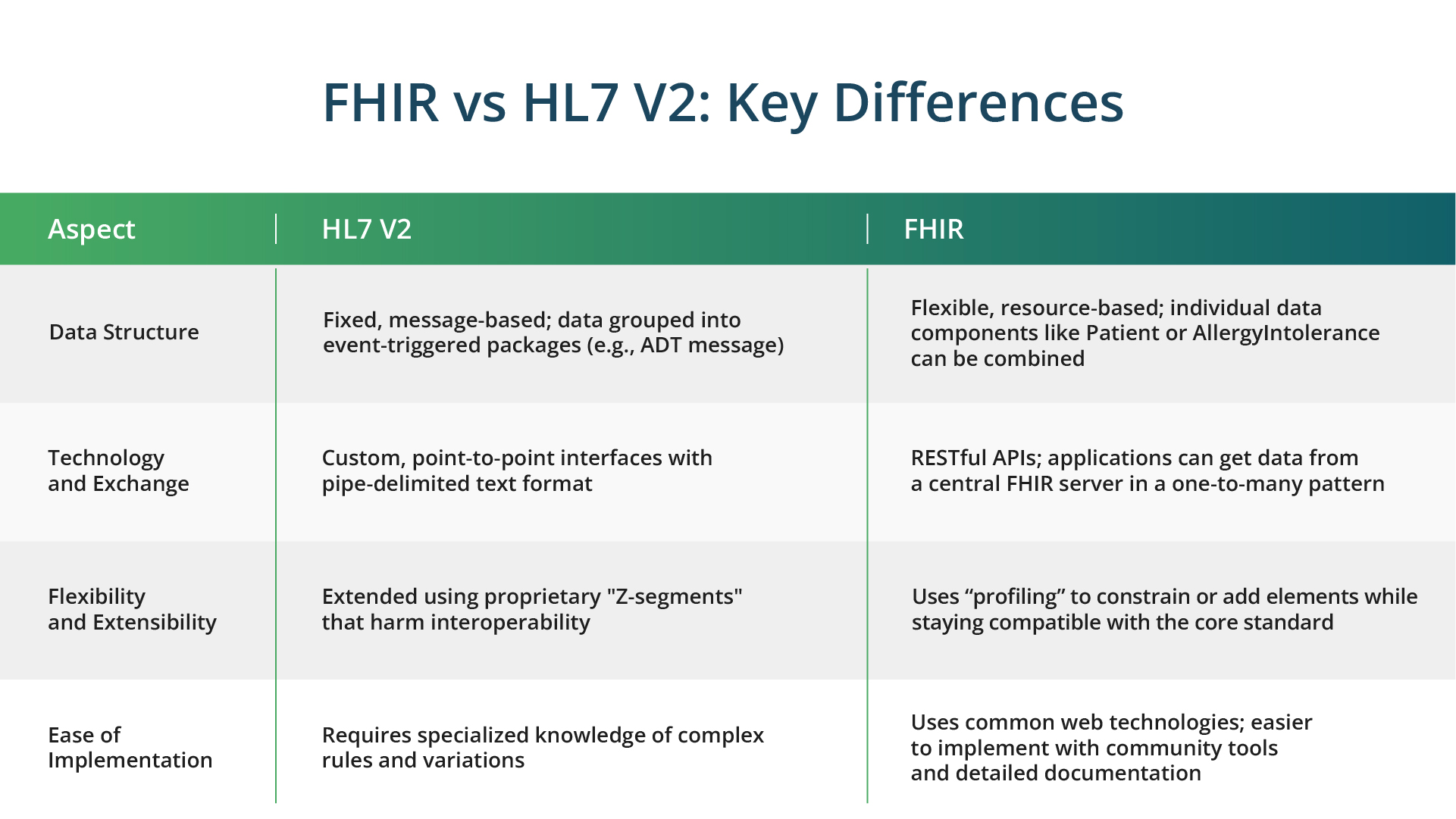
While both standards work toward interoperability, their methods are completely different.Data Structure
HL7 V2 uses a fixed, message-based structure where data is grouped into event-triggered packages (like an ADT message). FHIR employs a flexible, resource-based model where individual data components (like Patient or AllergyIntolerance) can be queried and combined as needed. This change from a document-centric to a data-centric model enables more specific and contextual data access.Technology and Data Exchange
HL7 V2 depends on custom, point-to-point interfaces and a complex, pipe-delimited format. FHIR uses modern RESTful APIs, which let any authorized application get data from a central FHIR server in a one-to-many pattern. This API-driven method is standard on the modern internet and helps make data exchange smoother and more scalable.Flexibility and Extensibility
Extending HL7 V2 usually involves proprietary "Z-segments" that harm interoperability. FHIR is designed for extensibility using "profiling," a standard method for constraining or adding elements to a resource for a specific purpose while staying compatible with the core standard. This approach allows local needs to be met without losing interoperability.Ease of Implementation
Implementing HL7 V2 demands specialized knowledge of its complex rules and variations. FHIR is much more accessible to a wider range of developers because it uses common web technologies. Its documentation is thorough, and a large community provides open-source tools and support, which cuts down on implementation time and cost.
What are the key use cases for each standard?
The technical differences between HL7 V2 and FHIR make them right for different jobs.HL7 V2 Use Cases
HL7 V2 is still the standard for essential internal tasks in established healthcare facilities. Its primary uses include:- Integrating Legacy Hospital Systems: Connecting EHRs with laboratory (LIS), radiology (RIS), and billing systems that have used V2 for decades.
- High-Volume Internal Data Feeds: Sending admissions, discharges, and transfers (ADT), orders, and results within a single hospital.
FHIR Use Cases
FHIR's flexibility and web-based design open up a much wider set of possibilities, especially for external data exchange and modern apps. Key uses include:- Mobile Health Applications: FHIR is the engine behind patient portals and mobile apps that give patients real-time access to their lab results, medication lists, and appointments.
- Inter-Organizational Data Sharing: It allows for seamless data exchange between different hospitals, clinics, and payers within an Integrated Care System (ICS) or Health Information Exchange (HIE).
- Clinical Decision Support System (CDSS): FHIR can supply real-time patient data from multiple sources to CDSS tools, giving clinicians timely and relevant alerts and recommendations.
Real-World Example: Integrating Health and Social Care with FHIR
The UK's National Health Service (NHS) provides a strong example of FHIR's capabilities. The Interweave platform, an NHS-owned shared care record system, uses FHIR as its foundation to address a complex problem: integrating health data with social care data. Social care services frequently use unstructured narratives instead of coded data, which makes interoperability with clinical systems difficult. Terminology also differs; an "episode of care" in a hospital means something very different than it does in a social services setting. To address this, Interweave formed a working group of health experts, social care professionals, and FHIR specialists. Their approach involved:- Defining a Minimum Viable Dataset (MVD): The group pinpointed the most critical data elements that had to be shared between health and social care.
- Creating Custom FHIR Profiles: Since a one-size-fits-all model would not work, the team developed a separate FHIR profile for a social care "Episode of Care." This adapted the standard to fit real-world social care situations while remaining FHIR-compliant.
What Does the Future Hold for HL7 and FHIR?
The healthcare industry is transitioning. FHIR is the clear standard for the future, pushed by regulations like the 21st Century Cures Act. However, HL7 V2's massive installed base means it will stay relevant for years. The challenge for most organizations is not choosing one over the other, but managing how they coexist. This situation has created a demand for HL7 V2 to FHIR transformation solutions. The process is complex because it involves carefully mapping V2's segment-based structure to FHIR's resource-based model and handling organization-specific customizations. The FHIR ecosystem is set to expand. Programs like SMART on FHIR are creating a "plug-and-play" environment for health apps, so developers can build one application that runs securely on any FHIR-enabled EHR. The standard is also evolving to handle genomic data and support advanced AI and machine learning models, which will lead to more predictive and personalized medicine.How Can Kanda Help?
Handling the complexities of HL7 V2, FHIR, and the transition requires deep technical skill and strategic planning. Integrating legacy systems, ensuring data privacy, and mapping inconsistent data formats are major hurdles for many healthcare organizations. A partnership for custom software development can be invaluable.- Build Custom FHIR Platforms: Develop secure, scalable, and compliant FHIR servers and APIs designed for specific organizational needs.
- Manage Legacy System Integration: Create effective data transformation pipelines to convert HL7 V2 messages into FHIR resources, bridging the gap between old and new systems.
- Develop Interoperable Applications: Design and build patient-facing mobile apps, clinician decision support tools, and analytics dashboards that use the full power of FHIR.
- Ensure Security and Compliance: Engineer platforms to meet strict regulatory rules like HIPAA and GDPR, protecting sensitive patient information at all times.
Conclusion
The shift from HL7 V2 to FHIR mirrors the broader change in healthcare from siloed, institution-focused systems to a connected, patient-centered ecosystem. HL7 V2 continues to be a crucial standard for internal data exchange, but its architecture belongs to a past technological era. FHIR, with its modern, web-based foundation, is the future, providing the flexibility, scalability, and developer-friendliness needed to drive innovation. For healthcare organizations, the path forward isn't about replacing everything at once but about smart integration. The key is to build a strategy that uses the strengths of both standards. This creates a bridge from legacy systems to the interconnected possibilities of the future. By adopting modern standards like FHIR, the healthcare industry can unlock the full potential of its data to provide safer, more efficient, and effective care for everyone.Related Articles

Healthcare Web Development: The Fastest Route to Scalable Patient Care
Outdated medical software is becoming a rising problem for healthcare facilities across the US, yet the push for digital patient experiences continues to grow. A CDC study found that 47.7% of adults ages 30-44 use the internet to communicate with a doctor or doctor's office. However, still existing paperwork, manual processes and legacy systems prolong…Learn More
RPA in Healthcare: Smarter Operations for Better Patient Care
The healthcare industry today is not only struggling with growing administrative spending but also with the increasing rates of staff burnout in healthcare facilities due to the high volume of repetitive tasks. As per Statista, 58% of registered nurses report burnout on most days, which results from both excessive emotional stress, the growing workload and…Learn More
Conversational AI for Healthcare: Changing How Patients Experience Care
The U.S. healthcare system has a serious problem with communication and management. Much of the strain comes from staggering administrative burdens. Research shows that physicians may spend nearly half of their clinic day devoted to documentation and non-clinical work. This imbalance damages the quality of care, makes it harder for people to access help, and…Learn More
Health Insurance Software Development: AI for Prior Authorization
Prior authorization (PA) was supposed to serve as a safety net, checking that patients get the right treatment while keeping costs in check. In reality, it now sits among the biggest administrative hurdles in healthcare. The contrast is stark when you consider how fast the market is growing. The U.S. healthcare software-as-a-service sector was worth…Learn More