
May 06, 2026
Healthcare
Unlocking Actionable Insights from Medical Data with Clinical NLP
Key Takeaways
A 2024 systematic evaluation of clinical NLP pipelines found that up to 80% of the electronic medical record may be unstructured. That creates problems on several fronts. An AHRQ evidence review links documentation burden to burnout and EHR-related workload, while ONC’s USCDI program continues to expand the types of clinical notes that health IT systems need to exchange and use.
Clinical NLP closes that gap by turning text into structured, usable signals without forcing clinicians to document everything twice.
What makes it valuable is context. A production-ready pipeline should distinguish the difference between "asthma," "rule out asthma," "history of asthma," and "father has asthma." It should recognize whether a medication is current or discontinued, whether a symptom is patient-reported or clinician-observed, and whether a finding belongs to the current encounter or a prior one.
That contextual reasoning is what makes more accurate analysis of clinical documentation, patient data, and health records possible.
A few figures make the business case clearer:
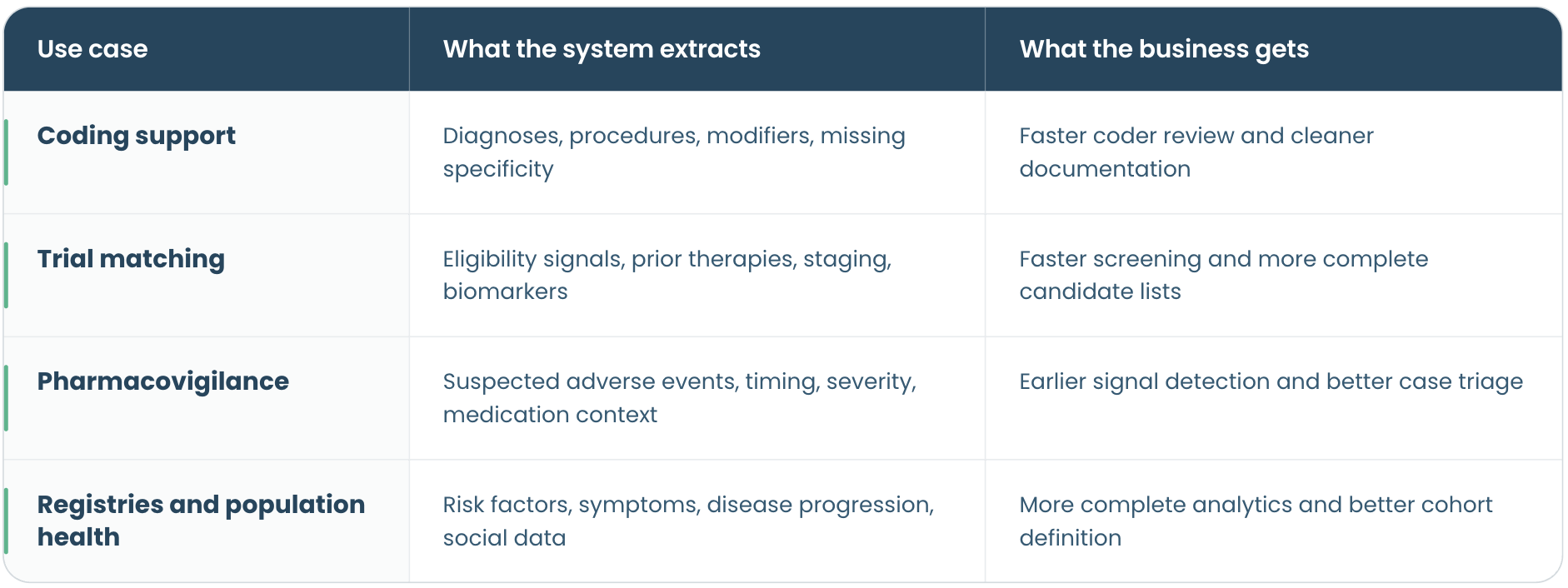
The tasks below are where teams usually see value first because they improve speed, consistency, and visibility without forcing clinicians to change how they document.
The tool choice also has to leave room for model calibration. Clinical NLP rarely works well with one universal confidence threshold across every task. A trial-matching workflow may prioritize recall so fewer eligible patients are missed, while coding support may need higher precision to avoid creating unnecessary review work. Teams should test models on local note types, tune thresholds by use case, and decide which outputs can flow downstream automatically and which need human review.
This requires a few practical standardization steps. Extracted terms should be normalized to accepted vocabularies: SNOMED CT for clinical concepts, RxNorm for medications, LOINC for labs, and ICD-10-CM for coding or reporting. Teams also need consistent rules for units, dates, negation, uncertainty, confidence scores, and source-note references so each extracted signal is easier to validate, audit, and reuse across analytics, EHR integration, and FHIR-based workflows.
Bias also deserves serious attention. Documentation styles differ by institution, specialty, clinician, and patient population. A model trained on one health system’s notes may underperform on another’s. For this reason, clinical NLP is strongest when it structures and prioritizes information for human workflows, not when treated as a fully autonomous decision-maker.
Best practices include:
The teams getting the most from it are not trying to extract everything at once. They choose a narrow, high-value workflow, map outputs to standards, keep humans in the loop, and measure what changes downstream. This is how clinical NLP moves from an interesting demo to something that improves coding throughput, trial recruitment, safety monitoring, analytics quality, treatment effectiveness, and ultimately, patient outcomes.
- Clinical NLP extracts useful details from notes, reports, and other free-text records so teams can work with them.
- The clearest use cases include coding support, trial matching, safety monitoring, registry work, and population health.
- The output is only useful if it connects to the standards healthcare teams already use: SNOMED CT, RxNorm, LOINC, ICD-10-CM, and FHIR.
- Accuracy depends on more than the model itself; teams still need calibration, human review, and ongoing monitoring.
- Clinical NLP reduces manual review and makes important information easier to find.
A 2024 systematic evaluation of clinical NLP pipelines found that up to 80% of the electronic medical record may be unstructured. That creates problems on several fronts. An AHRQ evidence review links documentation burden to burnout and EHR-related workload, while ONC’s USCDI program continues to expand the types of clinical notes that health IT systems need to exchange and use.
Clinical NLP closes that gap by turning text into structured, usable signals without forcing clinicians to document everything twice.
What Is Clinical NLP and Why Does It Matter?
Clinical NLP uses natural language processing, or natural language processing NLP, to extract meaning from medical text and convert it into structured data. In biomedical informatics, that usually means combining entity recognition, assertion detection, relation extraction, temporal interpretation, and terminology mapping so unstructured data becomes usable across systems.What makes it valuable is context. A production-ready pipeline should distinguish the difference between "asthma," "rule out asthma," "history of asthma," and "father has asthma." It should recognize whether a medication is current or discontinued, whether a symptom is patient-reported or clinician-observed, and whether a finding belongs to the current encounter or a prior one.
That contextual reasoning is what makes more accurate analysis of clinical documentation, patient data, and health records possible.
A few figures make the business case clearer:
- An IJERET study on an NLP-based medical coding system reported a 70% reduction in claim processing time and a 23% improvement in coding accuracy.
- ONC’s USCDI updates show that clinical notes are playing a growing role in interoperable health data exchange, which makes it more important to turn narrative documentation into usable structured data.
- A JAMIA study on automated trial eligibility screening found that NLP-based prescreening reduced coordinator workload by more than 90% and increased screening efficiency by 450%.
- A 2023 systematic review of AI for cancer trial enrollment found that every included study reporting time savings observed meaningful efficiency gains versus manual screening.
How Clinical NLP Brings Clarity to Health Data Governance
Clinical NLP is not only an extraction tool; it is also a governance tool when implemented with the right controls. For healthcare organizations, it turns fragmented health data into meaningful insights that teams can use.- It makes hidden information queryable. Symptoms, diagnoses, procedures, medications, and social factors once buried in narrative notes can be pulled into governed datasets for analytics, quality work, and operational follow-up.
- It reduces duplicate abstraction work. A single extraction layer can support coding, registries, care management, research, and reporting instead of having each team review the same charts separately.
- It improves data consistency. When extracted concepts are mapped to SNOMED CT, ICD-10-CM, RxNorm, or LOINC, organizations rely less on local shorthand and make downstream reporting easier to compare across departments and sites.
- It supports interoperability. Normalized outputs can move into warehouses and FHIR-based workflows instead of staying trapped in documents or PDFs.
- It strengthens trust and oversight. Teams can tie source-note references, confidence scores, versioning, and human review to each extracted signal, simplifying validation and audit trails.
- It narrows unnecessary access to raw notes. Instead of exposing every downstream team to full clinical text, organizations can share only the structured elements a workflow needs.
Key Tasks Clinical NLP Can Perform on Unstructured Clinical Text
Clinical NLP can handle many tasks, but the strongest use cases share one trait: they turn clinically important details buried in unstructured text into outputs another workflow can use. This includes free-text clinical notes, discharge summaries, and specialty documents healthcare professionals rely on daily.The tasks below are where teams usually see value first because they improve speed, consistency, and visibility without forcing clinicians to change how they document.
Named Entity Recognition, Information Extraction, and Terminology Mapping
NER identifies clinically important spans of text such as diagnoses, symptoms, medications, procedures, anatomical structures, lab values, and social risk factors. In practice, it extracts specific entities from unstructured clinical text and maps them to standard vocabularies. This ensures clinical information is reusable – "MI," "heart attack," and "myocardial infarction" all resolve to the same concept.Assertion, Context, and Temporal Information Extraction
This is what keeps extraction clinically useful. A pipeline has to know whether a finding is present, absent, suspected, historical, family-related, or tied to another encounter. In other words, it has to capture time, certainty, and source so the right relevant information is attached to the right patient conditions. Without that layer, even strong entity extraction can produce unsafe analytics and noisy downstream workflows.Automated Medical Coding and Revenue Cycle Optimization
Coding support is one of the clearest business cases for clinical NLP. Models can review narrative documentation, suggest likely diagnoses and procedure-related concepts, and surface missing specificity before claims move downstream. This does not remove coders from the process; it reduces administrative burden for healthcare providers by shifting the workflow from reading every chart from scratch to reviewing prioritized, structured suggestions.Clinical Trial Matching, Eligibility Criteria, and Patient Cohort Identification
Trial matching works well with NLP because many eligibility signals live in text: prior therapies, staging, biomarkers, response history, and exclusion criteria. In the JAMIA eligibility screening study, automated screening cut the number of encounters needing manual review from roughly 98 to eight per trial on average.Adverse Event Detection and Pharmacovigilance
Medication-related safety signals often appear first in narrative documentation. Clinical NLP helps teams scan notes for possible adverse drug events, triage them for review, and feed structured safety workflows. The FDA’s PrecisionFDA adverse event challenge explicitly frames NLP as a way to accelerate extraction of symptoms and key features from narrative text.Registry Abstraction, Patient Data, and Population Health
Another strong use case is pulling clinically meaningful facts into registries, quality programs, and operational dashboards. Smoking status, disease severity, functional status, complications, social determinants, and patient demographics are often documented in notes long before they are normalized elsewhere. This makes it easier to connect narrative text to broader patient data in real world settings.Where Clinical NLP Delivers Value
Building a Clinical NLP Pipeline: Architecture, Data Science, and Implementation
Clinical NLP does not need to start as a giant platform. It needs a workflow that can prove value, a governed data path, and trustworthy output. In the healthcare industry, the best implementations typically solve one problem well before expanding.Definition of Use Cases
Start with one operational problem, not one model. A coding assistant, a trial-matching engine, and an adverse-event detector all use clinical NLP, but they require different note types, thresholds, and validation paths. The best starting point is one use case, one owner, and one success metric.Data Preparation for Large Volumes of Unstructured Data
The most expensive mistake is treating all notes the same. Progress notes, pathology reports, radiology reports, and emergency department notes behave differently, especially when teams are dealing with large volumes of unstructured data. Good preparation usually includes selecting the right note types, removing duplicates, segmenting sections, and deciding which signals must become structured outputs.Selection of Technology, NLP Tools, and Model Calibration
There is no single best toolset. Open-source options such as Apache cTAKES, medspaCy, and scispaCy appeal to teams that want flexibility and have in-house engineering capacity. Managed or commercial options such as Amazon Comprehend Medical and John Snow Labs’ healthcare tooling make sense when speed, packaged healthcare functionality, and support matter more than full control.The tool choice also has to leave room for model calibration. Clinical NLP rarely works well with one universal confidence threshold across every task. A trial-matching workflow may prioritize recall so fewer eligible patients are missed, while coding support may need higher precision to avoid creating unnecessary review work. Teams should test models on local note types, tune thresholds by use case, and decide which outputs can flow downstream automatically and which need human review.
Data Ingestion and De-Identification
Before model work begins, the ingestion path must be clean and defensible. Notes may arrive through HL7 messages, FHIR APIs, document feeds, or direct EHR extracts. Whatever the path, access controls, logging, and de-identification need to happen early. HHS guidance on HIPAA de-identification makes it clear that covered entities generally rely on Safe Harbor or Expert Determination.Interoperability Through Standardization
Extraction is only half the job. Teams also need a place for the output to live. Clinical NLP becomes far more useful when mentions are mapped into standard vocabularies and written into interoperable targets such as FHIR Observation, FHIR MedicationStatement, or FHIR AdverseEvent resources.This requires a few practical standardization steps. Extracted terms should be normalized to accepted vocabularies: SNOMED CT for clinical concepts, RxNorm for medications, LOINC for labs, and ICD-10-CM for coding or reporting. Teams also need consistent rules for units, dates, negation, uncertainty, confidence scores, and source-note references so each extracted signal is easier to validate, audit, and reuse across analytics, EHR integration, and FHIR-based workflows.
Deployment, Monitoring, and Continuous Improvement in Real World Settings
Clinical language changes constantly. Templates change, specialties use different shorthand, and documentation habits drift over time. Mature NLP systems track more than model scores; they monitor reviewer overrides, agreement rates, exception queues, specialty-level drift, and whether users trust the outputs. In most deployments, the most significant and resource-intensive parts are not just inference – they are integration, privacy review, terminology mapping, and human validation.Compliance, Privacy, and Ethical Considerations in Clinical NLP
Clinical NLP requires the same discipline as any other healthcare data program, with extra attention to free text. Notes often contain names, dates, locations, and incidental identifiers not exposed by structured systems. De-identification, minimum-necessary access, role-based controls, and audit logging should be built in from the start.Bias also deserves serious attention. Documentation styles differ by institution, specialty, clinician, and patient population. A model trained on one health system’s notes may underperform on another’s. For this reason, clinical NLP is strongest when it structures and prioritizes information for human workflows, not when treated as a fully autonomous decision-maker.
Best practices include:
- Testing models across different note types, departments, and patient groups.
- Reviewing false positives and false negatives with clinical or operational experts.
- Keeping humans in the loop for high-impact outputs such as diagnosis support, safety review, or trial eligibility.
- Monitoring performance drift as templates, documentation habits, and patient populations change.
- Preserving confidence scores, audit trails, and source-text references.
The Road Ahead: Clinical NLP, Large Language Models, and Retrieval-Augmented Generation
The next phase of clinical NLP is not replacing everything with a general LLM. It involves using better domain-tuned models—including LLMs and deep learning models trained on biomedical literature inside safer, more controlled workflows. It is also where retrieval-augmented generation belongs and where traditional NLP methods remain the better fit. One clear trend is the growth of medically tuned language models such as Google’s Med-PaLM and Med-PaLM 2 research, Microsoft’s BioGPT, and the ClinicalT5 line of research. Another is multimodal work combining notes with imaging, pathology, and lab context, as seen in Google’s multimodal medical AI research. A third trend is privacy-preserving learning. In a 2024 evaluation of federated learning for biomedical NLP, federated approaches outperformed local-only training on the evaluated tasks. On the operational side, near real-time clinical NLP is making it more realistic to support action while the workflow is still moving.How Kanda Can Help
Clinical NLP projects often stall for predictable reasons: the model works in a demo but not in the workflow, integration takes longer than expected, or governance arrives too late. This is where the right engineering partner matters, especially when clinical applications must be reliable in production. Kanda can help by combining AI and machine learning services, healthcare software development expertise, and data and analytics capabilities to turn narrative records into usable business and clinical signals.- Build clinical NLP solutions around a specific outcome, such as coding support, registry abstraction, trial matching, or safety signal detection
- Connect NLP outputs to EHR integration workflows and healthcare interoperability strategies
- Map extracted concepts into analytics-ready data products that support reporting and predictive modeling in healthcare
- Extend clinical NLP into life sciences workflows tied to drug development and laboratory automation
- Design governed pipelines with privacy controls, terminology mapping, interoperability, and monitoring built in from the start
Conclusion
Clinical NLP is no longer a niche research topic. It is a practical way to unlock value from the part of the medical record that structured fields still miss – whether that means better analytics, stronger clinical practice, or more informed medical research.The teams getting the most from it are not trying to extract everything at once. They choose a narrow, high-value workflow, map outputs to standards, keep humans in the loop, and measure what changes downstream. This is how clinical NLP moves from an interesting demo to something that improves coding throughput, trial recruitment, safety monitoring, analytics quality, treatment effectiveness, and ultimately, patient outcomes.
Related Articles

CMS Prior Authorization Rule 2026: What Health Systems and Payers Actually Need to Build by October 2027
Key Takeaways The 2026 CMS Prior Authorization (CMS-0062-P) rule extends electronic prior authorization requirements to drugs for the first time, closing a major gap left by the 2024 rule. The hard compliance deadline is October 1, 2027 - by that date, systems must be live, not in development or testing. Compliance requires three major technical…Learn More
Why Omics and Clinical Data Integration Remain a Challenge and How to Fix It
Key Takeaways Omics and clinical data often remain separate, making them harder to use together than they should be. The main challenge is usually not the data itself, but the mismatched formats, siloed systems, and disconnected teams surrounding it Addressing that requires robust infrastructure, shared standards, and workflows that hold up without constant manual intervention.…Learn More
AI Copilots in Healthcare: Minimizing Diagnostic Risks With Smart Virtual Assistants
Key Takeaways AI copilots act as always-on virtual assistants managing documentation, triage, and decision support so clinicians can focus on patients. With 12 million diagnostic errors and up to 80,000 deaths annually, AI copilots are built to catch what overloaded clinicians miss, not replace them. Dragon Copilot saves clinicians around 5 minutes per encounter with…Learn More
Change Management in Healthcare Software: The Missing Piece of Digital Transformation
Key Takeaways Nearly two-thirds of healthcare change projects fail, and the root cause is almost always people and process, not technology. Clinician resistance is a rational response to workflow disruption, not a personality problem. Plan for it. Change management is a parallel workstream that runs alongside software development from day one, not a training session…Learn More

